January 2007 Monthly Archive
When Your Patient's Parent Is A Psychiatrist and A Patient and You Just Want To Go To Bed
If you want to test the faith of a psychiatrist in their "science", present them with one of their own.
In my career I have treated a few dozen children/spouses of doctors, and about a dozen of psychiatrists. Treating patients with these connections is difficult, if we are to be honest, for two reasons: 1) a lot of the trickery and hand waving we use on regular patients won't work with them, because they know the game. 2) we feel tremendous pressure to do a good job, because we feel that we are being graded.
The result is we almost always do an inferior job. Notwithstanding the admonition against treating family, the reality is that if they knew what to do, they wouldn't be referring them to you. And the trickery and bs are vital parts of the dance: these say you have really no idea why this works, but you're optimistic, so you are offering a framework to think about how it could work. The framework doesn't have to be "true"-- it has to be internally consistent.
But the countertransference towards the patient and his family is so strong that we do things we should not, think things we should not.
Treatment is even harder when both the patient's psychiatrist-parent/spouse is also a psychiatric patient somewhere. If you want to see an entire department blow an aneurysm simultaneously, say, "I'm getting X as a patient, and X's mom is a psychiatrist-- and a patient in the Bipolar clinic!"
In any other scenario, a mom in the bipolar clinic would suggest that the child had a similar disorder, by virtue of being a first degree relative. But in these cases, psychiatrists read it differently: it means the mom made the kid insane. It was the mom's fault. Not genetics, or biology, or even shared environment: specifically bad parenting. And not bipolar-- personality disorder.
I can make a statement that is completely unqualified, without exception: never, not once, has anyone hearing of this scenario said to me something like, "bipolar in educated families is difficult to treat." In every case, again without exception, every single person who has heard of the situation has said the same exact thing: "Oh my God, she's a borderline, and the mom is even more crazy."
What's interesting about this, to me, is two things. First, how immediate, reflexive, and certain everyone is of this assessment-- given even before they ever see the patient, only hearing that the mother of a patient is a psychiatrist. "Mom's a psychiatrist..." Boom. Case closed. Out the window goes diagnosis, biology, serotonin, kindling, TSH, whatever-- it is immediately predicted to be personality disorder due to an unhealthy relationship between parent and child (or spouses). Overinvolved, underinvolved, abusive, manipulative, whatever.
Medications are inevitably thought of as band-aids-- likely to be changed thousands of times over the lifetime-- or proxies for therapeutic maneuvers ("I will nurture you by giving you extra Klonopin to get you through the holidays, but then I will be a disciplined parent-surrogate and reduce it in January.") A family history of CNS lymphoma is less telling than a Dad who is a psychoanalyst. The adult child is crazy because the parents made him crazy.
That's the first thing. The second thing is this: they are almost always right.
More in next post.

 Score: 1 (1 votes cast)
Score: 1 (1 votes cast)
Atkins v. Virgina and the Execution of the Mentally Retarded
Once again, I appear to be all alone.
...Because of their disabilities in areas of reasoning, judgment, and control of their impulses, however, [the mentally retarded] do not act with the level of moral culpability that characterizes the most serious adult criminal conduct... [over the past 13 years the] American public, legislators, scholars, and judges have deliberated over the question whether the death penalty should ever be imposed on a mentally retarded criminal. The consensus reflected in those deliberations informs our answer...
So opens Atkins v. Virginia, as opined by Justice Stevens.
It seems unassailable that the mentally retarded should not be executed. Justice Stevens spoke of a consensus; the APA's amicus brief to the Court stated:
(1) there is a clear and unmistakable national consensus against the imposition of the death penalty on persons with mental retardation, and (2) the American people oppose the execution of individuals with mental retardation because the practice offends our shared moral values. (emphasis mine.)
So once again I am the sole hold out to national consensus. Okay. If I am to grant that such a national consensus does exist-- which it most obviously does not-- it is not in small measure due to misunderstanding what mental retardation is: it isn't Down's syndrome. It isn't a guest spot on the Howard Stern Show, it isn't finger paints and a baseball cap at age 30 moaning, "I wanna eat tato chips!"
If it was this, I'd agree a consensus might even be close to unanimous. Ironically, such a consensus would be irrelevant as such individuals don't commit capital offenses.
But this is not what mentally retarded is. Atkins, the above defendant, was determined by the defense expert to be MR because of an IQ of 59. With this IQ, he was able to get drunk and smoke pot (which, FYI, does not diminish responsibility,) drive a car (which he was licensed to do), kidnap and drag his victim to an ATM to force him to withdraw $200, then drive him to an isolated spot and shoot him 8 times-- not to mention be competent to stand trial, cooperate in court and with his attorney, etc. He was also able to pull of 16 other felonies in his life. An IQ of 59 allows reading at a 6th grade level-- comic books are 4th grade and Time Magazine is 9th grade.
But that was Atkins. A diagnosis of MR is an IQ less than 70. Can someone with an IQ of 70 appreciate that shooting your kidnapping/robbery victim in the chest 8 times and dumping him in an isolated location is really, really, wrong? From 1976-2002, 44 people with "mental retardation" have been executed; all but 2 had IQs at least 58.
So a categorical exemption for the mentally retarded might be sensible if someone could tell me exactly what mentally retarded means. Because the psychiatric definition quite obviously covers individuals well within competency standards. And that's the point.
Here's an example: if the exemption was for "Down's Syndrome" then this would be plausible, because a) we can reasonably agree how Down's impacts the defendant; b) we can identify it. But "retardation" means-- what? Mentally ill, as an exemption, is worse-- does depression count? Only psychosis? Does the presence of only a hallucination count, or do you have to have a thought disorder? "Schizophrenia?" What's that? The John Nash type, or the homeless crackhead type? How about borderline? Narcissism? If you can't be sure of what constitutes "mentally ill", how can you make a blanket exemption for it?
We can take this debate up a level, and observe that with every other psychiatric disorder that impacts on legal matters, the question for psychiatrists is simply, "what's his disorder?" or "how does the disorder impact this case?"-- we have an advisory capacity, leaving the ultimate decision of culpability up to the courts. In this way, we put some distance from the outcome. That's what expert testimony is all about. Fair enough. But now, with MR, the diagnosis automatically gets you out of execution. As long as the IQ test comes back 59, the sentence changes. Mental retardation is binary, apparently, and if you are fortunate enough to have it, you live-- regardless of how well you understood the wrongness of your actions, or how egregious were the crimes.
Which is ridiculous. There are practically no valid measures for any psychiatric illnesses-- everything is up for debate and interpretation. MR especially is a continuum disorder. Factors as trivial as which IQ test is used, or when it is taken, can affect the diagnosis. One study finds a 6 point increase using older tests vs. the newer version of the same test.
"Our findings imply that some borderline death row inmates or capital murder defendants who were not classified as mentally retarded in childhood because they took an older version of an IQ test might have qualified as retarded if they had taken a more recent test," Ceci says. "That's the difference between being sentenced to life imprisonment versus lethal injection."
But now the law has set an arbitrary and empty, binary cut off for execution. Psychiatrists now actually choose the sentence. Not inform the sentence-- choose it.
I'm fairly certain the APA didn't think about this when it filed its amicus brief. They never think these things through, because they believe they are an instrument of social change. But, like forced medication to render competent to be executed, psychiatrists have now boxed themselves into a corner. It is now solely up to them-- and their "tests"-- to decide who gets executed.
Consider the ethical dilemma for a forensic psychiatrist asked to evaluate for MR: given that the defendant can fake MR; and given that finding the defendant does not "have" MR--or suspecting that he is faking MR-- is exactly equivalent to sentencing him to death, can there be any other medically ethical outcome than finding they are MR? Think well. In other words, an answer is forced, an answer is created, simply by asking the question. The situation here is identical to the judge leaning over and asking, "Do me a favor and decide for me. Should I hang him or put him in prison?" Um, well, gee, it's up to me? um, since you asked...
I know, doctors are going to inwardly smile, pat themselves on the back for their cleverness; after all, the goal is to abolish the death penalty for everyone, one group at a time. And I am sure there are organizations who will actively, openly, exploit this loophole.
Notwithstanding the laudability of this goal, this isn't about the death penalty, it's about who decides the death penalty.
Just remember, when society allows psychiatrists to decide who lives or dies, then psychiatrists will also decide who dies or lives. I want everyone on the planet to take a very deep breath, and think about this.
Score: 2 (2 votes cast)
Further Thoughts on Competency To Be Executed
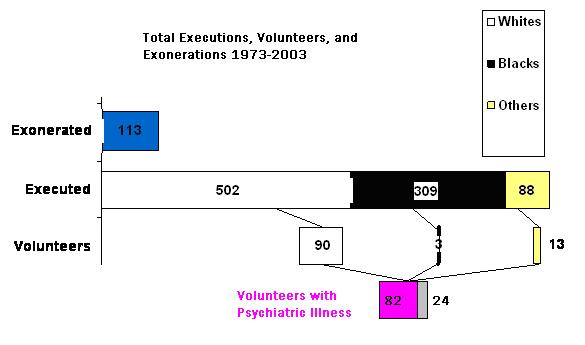
I took the data in the paper "Killing the Willing: "Volunteers," Suicide and Competency" and drew this chart.
The paper is fascinating. It observes that although blacks are disproportionately represented in executions versus the general population, volunteers to be execute-- i.e. people who waived their appeals-- are overwhelmingly white, male, and have psychiatric illnesses, especially borderline, depression, and psychoses (and an additional 10% have substance abuse)-- which is basically your demographic for suicide attempts. 30% also had prior suicide attempts.
So the author asks: if there is no such right to assisted suicide (indeed, any suicide at all), can there ever be a waiver of the appeal in capital cases? Even if the defendant is competent, if suicide is a motivation, the author writes, "their decisions should not, indeed must not, be honored, at least so long
assisted suicide is not available to other persons in the jurisdiction."
The counter argument, of course, is that competency is a legal matter, and the person's motivations beyond that are irrelevant. For example, if a guy is sentenced to prison and wants to go, he still goes.
McClesky v. Kemp (1987) attempted to abolish the death penalty under the argument that executions were influenced by racial discrimination. This was rejected. But Atkins v. Virginia (2002) did abolish the executions of the mentally retarded. Consequently, abolition of the death penalty, or at least a drastic curtailing of it, is more likely to occur along lines of competency and mental state, rather than any appeal to morality, race, or class.
I thought I knew how I felt about this issue, and now I am not so sure. But before anyone forms their opinion, I would strongly urge everyone to read the dissent by Scalia in the Atkins case. It should be required reading for every psychiatrist, whether you agree with him or not.
Score: 4 (4 votes cast)
Competency to Be Executed
If society has determined that a right to commit suicide does not exist, can a convict sentenced to death waive his appeal?
Continue reading:
"Competency to Be Executed" ››
Score: 4 (4 votes cast)
Competency To Commit Suicide?
Continue reading:
"Competency To Commit Suicide?" ››
Score: 3 (5 votes cast)
More on Medical Competency
The primary rebuttal to my thesis of personal autonomy is, "well, we doctors are just trying to do what's best for the patient." This is categorically false (words chosen carefully.) What they want is what's best for that particular medical issue because it leads to the betterment of the patient; but this is not the same as taking the patient's life in total and deciding what is best overall for their lives. What the patient wants in their lives may be, to them, worth the risk.
And I'm not saying the doctors aren't trying to do what they think is best; but you don't think George Bush, et al, are doing "what they think is best" for us? (Before you give a reflexive answer, grow up.) Allowing doctors extraodinary powers to treat against one's will is no different than executive privilege, an example chosen carefully because it highlights the political/societal nature of the process, over the scientific.
Continue reading:
"More on Medical Competency" ››
Score: 2 (2 votes cast)
Not Competent To Make Medical Decisions?
As a forensic psychiatrist, I am often called to evaluate someone for their "competency"-- to make medical decisions, to make financial decisions, to stand trial, and (theoretically) even to be executed.
In these various consults, the basic question is this: are they so impaired, that they don't understand the relevant issues and can't make rational decisions?
Many psychiatrists find this complicated and time consuming work, because they focus on the nuances of the patient's symptomatology and illness. They try to get extensive past histories, corroborating information, etc, etc. All this is important, but they miss the forest for the trees.
Now this is, of course, only my opinion. But it's important that you hear this opinion, because I am, apparently, the only person who has it, so you won't hear it anywhere else.
The truth to competency evaluations is this: the patient is the least important factor.
Continue reading:
"Not Competent To Make Medical Decisions?" ››
Score: 0 (0 votes cast)
Neither Is This Is A Narcissistic Injury
I have another unrelated post coming, but a quick word on insults vs. narcissistic injuries, and why this distinction is so important.
Narcissistic injuries have nothing to do with sadness. They are always and only about rage.
The narcissist says, "I exist." A narcissistic injury is you showing him that he does not exist in your life. Kicking him in the teeth and telling him he is a jerk is not a narcisstic injury-- because he must therefore exist.
Let's say I'm a narcissist, and you send me a 10 page letter explaining why I suck, I'm a jerk, I'm an idiot; you attack my credibility, my intelligence; and you even provide evidence for all of this, college transcripts, records from the Peters Institute, you criticize my penis size, using affidavits from past and future girlfriends-- all of this hurts me, but it is not a narcissistic injury.
A narcissistic injury would be this: I expect you to write such a letter, and you don't bother.
This is most easily seen in the failing marriage of a narcissist.
The reason it's important is because the reaction of the narcissist to either "insult" is different. In the first example, he will be sad and hurt, but he will yell back, insult you, or cry and beg forgiveness or mercy--he will respond-- maintain the relationship. He'll say and do outrageous things that he knows will cause you to respond again, to prolong your connections, even if they cause him misery. He doesn't care that it makes you and him miserable-- he cares only that there is a you and him.
But in the latter case where you ignore him, humiliate him-- an actual narcissisitic injury-- he will want to kill you.
----
And before everyone flames me, I am not trying to give a scientific explanation of the pathogenesis of narcissism. This is simply one man's opinion of how we can specify what it is, and what it may predict, past or future. Nor am I suggesting this isn't "treatable"-- anyone can change. It may not be easy, but it is always possible.
And I also do not mean to imply that all narcissists will kill everyone who injures them. The point is rage. They may never act on it, or they may break a window, or attempt suicide, etc.
Score: 9 (9 votes cast)
Borderline
Narcissism- what I believe to be the primary disease of our times-- is one side of a coin. The other side-- the narcissist's enabler-- is the borderline.
If the analogy for narcissism is "being the main character in their own movie," then the analogy for borderline is being an actress.
Continue reading:
"Borderline" ››
Score: 45 (49 votes cast)
Vote
Hi. Vote for me for Best Medical Blog.
Score: 0 (2 votes cast)
Xanax, Vicodin, Percocet, Ritalin and Valium
When patients complain about doctors, it's usually about overcharging and undercaring. When doctors complain about doctors, however, it's usually about those with "loose" practice, especially in the inner cities , who seem to overprescribe Xanax and Percocet.
But let's ask a different question: what would happen if all of these doctors disappeared? If there was no fast and easy way to get prescribed legal Xanax, would all the Xanax seekers just disappear?
In large part, many psychiatrists and primary docs have the luxury of proclaiming that they "don't give out Xanax and Percocet" because there is somewhere else for those patients to go. Dr. Smith from University Clinic doesn't have to haggle over #10 Percocets because the patients can go to other doctors who are much more-- comfortable, let's say-- giving out #90 Percocets a month.
I was trying to think of an analogy. Black market jumped to mind, but these items aren't illegal nor illegally obtained. Surprisingly, the best analogy I found was illegal immigration.
Continue reading:
"Xanax, Vicodin, Percocet, Ritalin and Valium" ››
Score: 7 (7 votes cast)
For more articles check out the Archives Web page ››