Presidential Anti-Pharma Rhetoric Heats Up
So once again I’m in the weird position of having to defend something I’m actually against.
The latest is from John Edwards, et al. Here’s the headline: Edwards unveils plan to control drug advertising.
Read that sentence, and decide what you think the intent of the plan is. Is he talking about controlling the colors of the ads?Most likely, you think it’s the effect the ads have on drug prices.
“The excessive costs of prescription drugs are straining family budgets and contributing to runaway health care costs…”
Let’s temporarily grant that that this statement is true. What is the link between advertising and prescription drug costs? Is he saying that spending on ads increases the price of drugs? That would be wrong, and I have to believe he knows it.
First, Pharma spends about $4b on DTC ads. It has yearly sales of about $200b, so even if every penny spent on ads was instead used to lower the price of the drugs, no one would actually notice. Additionally, prices of branded drugs rise about 6%/year, regardless of how much they spend on ads.
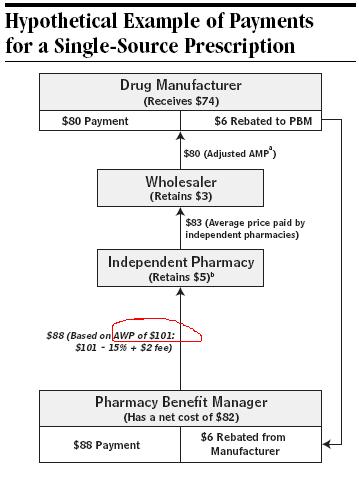
Second, we should probably define “drug prices.” If I roll into a pharmacy with a prescription and choose to pay cash, how much will it be? The answer, as it turns out, depends on the pharmacy. These are retail prices, that pharmacies charge no-insurance cash payers; on average, 15% more than insurance rates. But let’s be honest here: cash payers can’t afford a lot of these medications at any price. If you’re one of the unfortunate working poor who don’t have a prescription plan, you can’t afford the medication at full price, 20% off, even 50% off. The price is irrelevant; what matters is whether you have a prescription plan, or a doctor who can provide samples forever.
So for everyone else, “prices” really means prices to insurance companies, or Medicaid/Medicare, all who negotiate a price that has almost nothing to do with the actual patient demand for a drug. A price which is considerably lower than retail. Medicaid apparently gets a 20% discount, the VA 40%. (1)
So DTC advertising doesn’t affect the price because the consumer
isn’t paying it. The price was set in negotiation. Certainly the
price Pharma asks from wholesalers and insurers takes into account
their costs, including advertising; and more ads (hopefully) means more
scripts which means higher profits. But increases in advertising don’t
translate directly to higher prices, they reduce the profits. Higher
prices are the result of negotiations between parties that are
immune to the effects of advertising. That’s the problem.
Third: perhaps what we really mean is that DTC ads raise the overall Medicaid/Medicare expenditures because more scripts are being written that would otherwise not have been written without the DTC ads. Well, if this is what we’re saying, we should just say this; let’s not use factually inaccurate soundbites that play to the hearts of superficial idiots.
But if we are saying this, then the problem isn’t the prices of the drugs, it’s doctors prescribing drugs they shouldn’t be prescribing. The solution isn’t, therefore, to reduce drug prices; in fact, that’s the opposite of what you want, because it makes it even easier for doctors to prescribe what they shouldn’t be prescribing. The actual solution would either be to raise drug costs (bad idea), controlling doctors’ prescribing (bad idea), or giving them a medication budget they have to stay within, but preserving prescribing freedom.It should bring us pause that even the AMA refused to recommend banning DTC ads. If Edwards plan was specifically about protecting the patients from half-truths or seductive graphics that compel patients to request medications that they don’t need or might compromise their health, then I’m behind him 100%. I already think DTC should be banned. But like all political soundbites, this isn’t about content but about ambiance, creating a feeling that he’s all about cutting costs— that’s he’s more than Hillary. Unfortunately, empty rhetoric like this distracts us from real problems, like Iraq, Iran, wealth divergence, recession, etc.
——
1. As a horrifying diversion into drug pricing, let’s look at Medicaid.
Medicaid, by law, will pay (to a pharmacy who dispenses the drug) a percentage of the average wholesale price, plus a dispensing fee. Both the percentage and the dispensing fee vary from state to state, but it’s on the order of 85% of average wholesale price, and $5 dispensing fee. On average, Medicaid pays about $61 per prescription: $14 goes to the pharmacy, $47 to Pharma. If anyone can tell me how DTC ads affect that, I’m listening. So pharmacies don’t make a lot on this, and it’s a far cry from the markup the pharmacy can impose on a cash payer. And pharmacies aren’t obligated to participate in Medicaid.
In practice, wholesale price is anything Pharma says it is, including some bizarrely inflated price. But whatever it is, I hope it is clear that it has nothing to do with ads.
And then there are the rebates. I hope you’re sitting down.
In gratitude for this excellent reimbursement, Pharma agrees to rebate Medicaid about 15% or the manufacturer’s price, plus an additional rebate every year for the amount of price increase that exceeds inflation. In 2003, the average rebate was 31%.
There’s another rebate. Many insurances have pharmacy business managers (PBMs) who make preferred drug lists. How does a drug get on that list? It isn’t by being cheap; ask Illinois Medicaid in 2005, when they wouldn’t cover Seroquel, arguably the most demanded but hardly the most expensive. What it takes is, as they say in Big Pharma, “our willingness to play ball.” Another “rebate.”
That money stays in the managed Medicaid’s pocket. The savings aren’t passed on to the patient, either directly or indirectly. If you want an analogy, it’s the parking authority; revenue from tickets doubles, triples, but the amount they pay to the cities doesn’t change. The extra “profits” goes back into the authority, to hire more people, pay more salaries. It’s a self-propagating bureaucracy. I should also mention that, consistent with bureaucracies, it can’t even collect those rebates very well.
![]() Digg |
Digg | ![]() del.icio.us |
del.icio.us | ![]() StumbleUpon |
StumbleUpon | ![]() Reddit |
Reddit | ![]() Yahoo! |
Yahoo! | ![]() My favourites
My favourites
4 Comments