August 14, 2008
Seroquel For Bipolar Maintenance
A brief history of the past decade.
I. Background
A mood stabilizer is a drug that prevents mania and/or depression. Depakote was the default mood stabilizer since 2000. Hundreds of papers promoted its use, though all relied on a single double blind, placebo controlled trial as support for its efficacy. Mentioned almost no where was that this trial did not show any superiority over placebo. However, Depakote enjoyed tremendous sales in the years 2000-2008, showing 10-20% growth per year.
II. But the bulk of the support, especially in journals, came from academics who believed in it, not Pharma?
Since the academics have no relationship with Abbott and are motivated only by clinical efficacy, we can expect their promotion of Depakote to continue even after it goes generic. Oh, wait, that happens in 2008.
III. The Sad, Quiet Story Of The Mainetance Trial That Wasn't
Here's a quick summary of the (only) Depakote vs. placebo for maintenance study: manic patients were enrolled, put on Depakote + any other necessary meds until they were stabilized. Then these patients were randomized to Depakote, lithium or placebo.
At the end of the study, all three groups had similar relapse rates. Putting them on Depakote was not better than placebo for maintenance. On this single, failed trial, an entire decade of psychiatry was premised.
However, there is one technical point that I have never, not once, in 8 years, seen written about, discussed, or even alluded to, and when you do bring it up people look at you blankly: the study patients were stabilized on meds, then randomized to drug or placebo. So those that were randomized to placebo had their stabilizing meds stopped. They were "taken off their meds." So actually, being on Depakote was not simply no better than placebo, it was no better than abruptly going off your meds. Take a long hard look at yourselves.
IV. Two Drugs Are Better Than One
Depakote continued to be grow, continued to be a "mood stabilizer" when it was really simply an acute antimanic. NB: it may be true that Depakote is a tremendous mood stabilizer; you can't condemn the drug on one study. But, importantly, in the decade of "Evidence Based Medicine" why was it at the top of every treatment algorithm and guideline? There's the rub.
But psychiatrists did not use it as a monotherapy mood stabilizer-- it was always "mood stabilizer" plus something else. In fact, the major discussions in psychiatry 2001-2007 were whether/how additional medications would benefit when used with Depakote. No one asked whether Depakote itself was a mood stabilzier-- that was assumed. The question was whether adding antipsychotics to Depakote provided additional benefit. The answer was always "yes" as long as the question had the caveat, "notwithstanding details or generalizability."
Consider the study of Depakote alone, or Depakote + Risperdal, for the treatment of acute mania. Which is better?
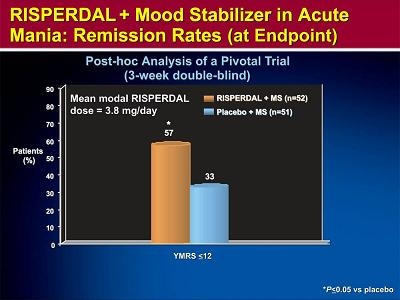
The graph is clear: the combination is better than the single drug alone. BTW, every atypical antipsychotic has a similar study with nearly identical results.
Two sleights of hand:
1. This is a study of acute mania--3 weeks-- not maintenance. The study does not say that Depakote + Risperdal will provide better maintenance control over a year. Yet that is how the results were generalized-- psychiatrists left their patients on "whatever" broke their mania. You can see how, over time, doses and number of meds keep going up.
2. See the y-axis? It doesn't say "amount of improvement," it says "percent of patients." It doesn't say that each person got more better, it says more people responded to two drugs than responded to one drug. We assume the superiority was the result of the combination. But how do you know it wasn't due entirely to the Risperdal? If you give a room full of manics Depakote, 25% get better. If you give a room full of manics Risperdal, 25% get better. If you gave both to everyone, then 50% would get better, but it's pretty clear that the Depakote responders didn't need Risperdal, and the Risperdal responders didn't need Depakote. Indeed, when you look at change of symptom severity, two meds was no better than more of one med.
This chart could simply be the result blasting patients with two drugs, hoping one works. So this doesn't say "if a drug fails, add a second." It says, "if a drug fails, switch to something else."
Which should have been so obvious as to never have necessitated a study.
V. So Then It's Agreed: Let's Change The Definitions So We Don't Get Caught
At some point, someone is going to notice that polypharmacy isn't working as promised; that it is not particularly safe; and that it certainly isn't worth the price.
And Depakote was going off patent. What to do?
What you do is write a completely unimpressive, pointless article (Effectiveness of Adjunct Antidepressant Treatment for Bipolar Depression) based on a multimillion dollar government finded study that tells us nothing we didn't already know for decades, in the most prestigious medical journal (NEJM) available, and in it sneakily and gigantically change the definitions of words to prepare for the next wave of psychopharmacology, granting plausible deniability.
Mood stabilizers were initially limited to lithium, valproate, the combination of lithium and valproate, or carbamazepine. In 2004, the protocol was amended to define mood stabilizers operationally as any FDA-approved antimanic agent.
Now, in two sentences, all the junk articles that used to apply only to Depakote can now be reused to apply to antipsychotics. "We've known since 2001 that mood stabilizers, for example Depakote or Seroquel or Abilify, are maintenance agents..."
VI. But How Can Antipsychotics Be Mood Stabilizers If They Are For Psychosis?
At first glance, the question seems reasonable, but for the fact that the none of the capitalized words above have any meaning at all, except those with three or less letters.
Seroquel for maintenance bipolar. Why not, a priori? Why would it be any worse than Depakote, a drug which didn't work anyway?
The problem, however, is that by pushing Depakote as a maintenance agent for so long, everything is reflexively considered second line, an add-on.
So because of the artifice, the semiotics, "bipolar requires mood stabilizers; Depakote is a mood stabilizer; bipolar needs Depakote" you can't do a Seroquel monotherapy study. It has to be done as an adjunct to Depakote or lithium. Therein lies the problem with the interpretation of the results.
The results are, indeed, impressive: people on both Seroquel and Depakote had fewer, and later, relapses than those on Depakote alone. This holds true whether you are looking at relapses into depression, mania, or all mood episodes.
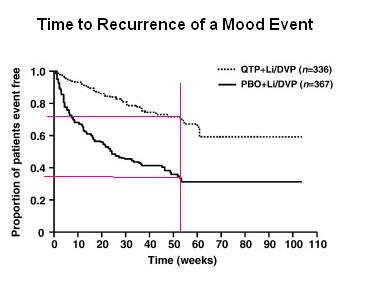
So, for example, by 52 weeks, about 25% of Seroquel + mood stabilizer patients had relapsed, while 62% of mood stabilizer alone patients had relapsed. That's an NNT of roughly 2.5, i.e. you need to put 2.5 people on Seroquel to reliably know one person benefited. Lipitor's NNT for reducing heart attacks is 25.
Although you're not supposed to compare results from different studies, I feel completely comfortable saying that the Depakote curve here is about the same as it was the in other maintenance study, i.e. no better than placebo. (Stop using Depakote.)
VII. But Is It Measuring Prophylaxis Or Relapse?
Look back at the Depakote study for a hint.
Patients were all stabilized on Depakote/Li with Seroquel over 36 weeks, and then randomized to either continuing Depakote/Li + Seroquel, or to being taken off Seroquel and being left on Depakote/Li. Those left on Seroquel did well; those who had the Seroquel removed did not.
So on the one hand, you could say "the combination prevented relapse," or, you could say, "abruptly stopping your Seroquel results in a relapse." Do you see the difference?
With the Depakote study, stopping your Depakote had no adverse effect. For whatever reason, stopping your Seroquel apparently does result in prompt relapse.
You are being tricked (not on purpose) by the presence of the Depakote, thinking that this is providing you some degree of mood stabilization, and the Seroquel is adding to it. Wrong. The Depakote is providing you nothing. The Seroquel is the mood stabilizer. And "stopping your meds" is, after all, not a good idea.
VIII. What Dose?
There is one other important result of this study. The patients were not simply on Seroquel; they were on Seroquel at fluctuating doses, per the judgment of the doctor, 400mg to 800mg. That is key. Seroquel didn't prevent relapse; rather, raising the dose whenever they needed it, and possibly lowering it when they didn't, is what kept them stable. Maybe if they were on a fixed dose of Seroquel the whole time, no opportunity to raise the dose, people would have relapsed more frequently. But this way, at the first sign of trouble, you pre-empt it by increasing the dose.
In other words, Seroquel didn't prevent relapse; prompt intervention by the doctor as things developed (using Seroquel) prevented the relapse. This doesn't diminish the utility of Seroquel, but it also doesn't mean you can put everyone on 600mg and say, "see you in a year."
That is, perhaps, why Depakote failed: it relied on a steady dose, titrated to an imaginarily important blood level that it seems never to have occurred to anyone to ask why we target.
IX. The King Is Dead, Long Live The King
Just as Depakote was an overhyped drug that will thankfully die with its patent, it is more than likely that Seroquel for maintenance bipolar disorder represents some sort of top in the antipsychotic market. It will enjoy massive, and steady, use for several years, but I doubt if there is much growth left in it. Astra Zeneca thinks it has penetrated a market; but it has really opened the doors for all antipsychotics in the same market. You can prescribe Seroquel; don't invest in it.
Simultaneoulsy, just as I was a vocal advocate for the use of antipsychotics over the massive overuse of Depakote-- and I thus contributed to the rise of Seroquel (and others), my new target may be the overuse of antipsychotics.
The target is not Pharma or reps, but academic physicians who are politicians posing as scienticians. Completely absent is the pursuit of science or truth-- e.g, "we didn't expect this result, I guess we were wrong"-- but diversions and sleight of hand. The point is not the results; the point is the discussion. The message doesn't matter, the medium is the message. They have an allegiance to a given concept, and they defend it, promote it. No different than a PAC. And when their King dies, they celebrate as if they never believed in him at all.
But at least the rise of Seroquel will benefit humanity in two important ways. First, it brings evidentiary support to the not common enough practice of fluctuating the doses as needed, up and down, rather than relying on a set dose.
Second, it means the demise of polypharmacy (until they invent a new class of drugs), the drastic reduction of the number of medications patients will be prescribed, especially when coupled with the slow demise of SSRIs.
![]() Digg |
Digg | ![]() del.icio.us |
del.icio.us | ![]() StumbleUpon |
StumbleUpon | ![]() Reddit |
Reddit | ![]() Yahoo! |
Yahoo! | ![]() My favourites
My favourites
29 Comments