April 2, 2009
This Is Why Medical Care Is Expensive
The article explains:
After we get home from setting a few car fires, we can then ask the relevant question: what, exactly, do they mean by "cost?" Do they mean "cost," or do they mean "bill?"
AUSTIN, Texas - Just nine people accounted for nearly 2,700 of the emergency room visits in the Austin area during the past six years at a cost of $3 million to taxpayers and others, according to a report.Activate populist outrage: ready, go!
The average emergency room visit costs $1,000. Hospitals and taxpayers paid the bill through government programs such as Medicare and Medicaid, Kitchen said.
After we get home from setting a few car fires, we can then ask the relevant question: what, exactly, do they mean by "cost?" Do they mean "cost," or do they mean "bill?"
I.
A frequent lament against the Obama bailout plans is that the taxpayers are footing the bill. Really? So your taxes have gone up?
Until they go up, you're not paying for nothing. The problem with the bailouts is precisely that our taxes haven't gone up: we're living on fake money again. If they had gone up, then we would be emotionally motivated to make real decisions about how we want to spend our money. In other words, once we start paying, we'll start to ask if it's worth what they billed.
II.
Healthcare may be the biggest racket in history. I don't mean it pejoratively. Quoting Charles Tilly: a racketeer is someone who creates a threat and then charges for its reduction.
This ER study can be translated: "holy crap, healthcare costs are spiraling out of control! Pay us, and we can fix it for you."
You'll see this in many forms, the most evident are this one, and electronic medical records.
Minimizing healthcare is the new healthcare.
III.
Focus on the cost: how did these patients rack up "an average of" $1000 per visit, exactly?
I once stood on a small hill and looked at an ER, and from what I could see with my B&L 10x binoculars, nothing that occurred there costed $1000. You might legitimately ask me who am I to judge what an ER visit costs; I'd submit that the only legitimate answer to what costs what is the market. But medicine isn't a market, because two parties don't agree to terms either by negotiation or by repeated bids and asks. One party makes up the terms, and the other party just pays it, or doesn't. Period.
College tuition is the same. I'm sure Harvard has some equation that spits out a $40k/year bill, but that number has no bearing on the actual costs. Case in point: if it did, they wouldn't suddenly be able to make tuition free for 20% of their students without gigantifying it for the other 80%. Perhaps tuition actually costs more than $40k. My point is that what we are asked to pay has very little to do with the actual cost.
Hospitals traditionally use the tuition model on patients: indigents can't pay, so Blue Cross is charged $300 for a guaze pad. Blue Cross knows perfectly well it is being "scammed" but they make it up from employer contributions, etc, etc, so no one complains. The only person who complains is an actual individual, with an income but no insurance, when he is asked to pay the Blue Cross rates. He doesn't realize he's being overcharged gigantically. He just knows he's about to go into bankruptcy. The problem simply is that he's caught in the healthcare racket that hospitals, the government, and private insurers have agreed to.
IV.
The article doesn't link the actual study, because the actual study is not available. Solid. I did find last year's study, which explained precisely how they arrived at the costs:
Calculating Estimated Costs
Because no cost data exist for charity care provided by ICC members, a method of estimating costs was selected based on a review of healthcare literature. The method chosen for this study, Diagnosis Cost Groups (DCG), uses patient diagnoses to estimate each patient's health status, or predicted need for healthcare utilization. The DCG models used all diagnoses from the one-year study period along with demographic patient data to calculate a measure of the expected costliness of each patient relative to the average Medicaid patient. This measure, called relative risk (RR), was then converted into annual patient cost estimates through the use of a cost multiplier. Once cost estimates were established, the RR scores were rescaled to have a mean of 1.0 by dividing each RR score by the mean RR score. The rescaled RR scores show how costly a patient is relative to the rest of the study population.
If you read something in a medical study that is confusing, it almost always means you are about to be misled. I'll translate this:
If the average Medicaid patient costs X, then each disease is weighted as a multiple of X. e.g. a diabetic patient "costs" 2X, according to the DCG.
It should be obvious that this number could as easily by 9X or .1X, or anything at all. Leave that aside.
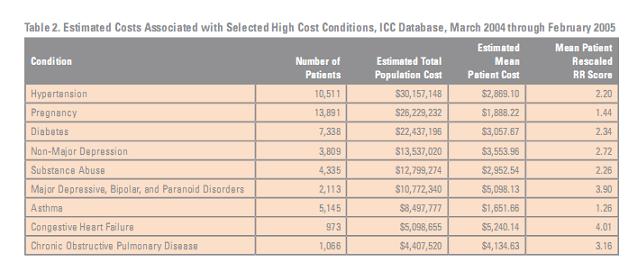
See how hypertension costs $30M to treat hypertension in the population? It doesn't. It costs $30M to treat all patients with hypertension and anything else they have. It doesn't cost $56M to treat pregnant hypertensives.

I'm sure this can easily be spun to mean "please give us more money so we can treat depression, because look how much it's costing you guys!" but it doesn't mean it costs $20M to treat depression, only that people with depression-- and all their other infirmities-- accounted for $20M. Of course, that's $20M in estimated costs, estimated by simply multiplying some hypothetical figure by 3.9.
Also note that even if we had the data for what each and every single patient spent that year, we'd still have no figure remotely close to the truth. $900 for an MRI? Please explain.
I had once read on the internet that price fixing was illegal, but I guess not.
V.
All of this comes down to the central issue in healthcare reform: reducing costs. Absolutely no one is seriously interested in doing this. They may be serious about reducing the billings to Medicare; or reducing the flow of money to Pharma-- all of which maybe legitimate goals. But these reductions in billings will inevitably be offset by increases elsewhere, because no one wants to get to the cost of anything. Aetna still needs to eat.
Aetna won't bother to cover anyone, and doctors wouldn't bother to treat anyone, if medicine billed what it costed. Unless a hospital can bill someone $300 for a guaze pad, it's going to close down and turn into a Dunkin Donuts.
Nor is the government interested in closing down Aetna or doctors; Medicare is social welfare program for medical providers, just as Medicaid is a social welfare program for the poor. The government will keep its books open, and pay the populace just enough to keep them from rioting.
Before you yell at me, understand why we're in this mess in the first place: because medicine is believed to cost the sum total of the physical capital-- procedures, guaze pads, and not the intellectual capital. (Lawyers have it the other way.) The solution to this is to value medical care as the actual cost (not billing) plus some reasonable amount for the intellectual thought that may go into it (assuming doctors agree to put some thought into it.) I'll add that $60 per patient from medicare is probably not going to be enough.
Certainly I am for "redirecting" the "frequent fliers." No argument from me that we spend money needlessly, that there aren't better alternatives. But don't be fooled for a second that anyone wants to implement the actual alternatives. We're going to spend money on electronic medical records.
Put another way: do you think those Austin area ERs will ultimately bill $3M less if they sent those 9 patients to Neptune? Let alone if they got Aetna?
![]() Digg |
Digg | ![]() del.icio.us |
del.icio.us | ![]() StumbleUpon |
StumbleUpon | ![]() Reddit |
Reddit | ![]() Yahoo! |
Yahoo! | ![]() My favourites
My favourites
12 Comments