April 24, 2009
What Should Count As A Disease?
Quick, look over there!
Ronald Pies writes:
and attempts an answer. It is this:
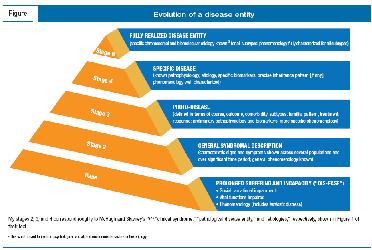
What exactly is a "mental disorder"? For that matter, what criteria should determine whether any condition is a "disease" or a "disorder"?
and attempts an answer. It is this:
I know you can't read the words in this graphic, but what's important is that his answer isn't an answer at all, it's another hierarchical model, not a physics-style concrete truth. Nothing the "Wovon Man" guy would sign off on.
This is not a failing of Pies; there's no possible way he could be expected to come up with a concrete solution. But his answer is just as ambiguous, relative, and subject to individual prejudices as simply defining a disease as "anything in which the person or surrounding people feel suffering. Severity of illness correlates to amount of suffering."
I'm not saying my definition is better-- it's equally valid, or invalid, or whatever you want to believe this whole project is.
It should be fairly obvious that "disease" is an entirely subjective term that can be applied legitimately to anything. "The disease of right wing conservative ideology." See? 50% of you agreed. Not jokingly agreed, mind you-- but found a serious element of truth to that diagnosis.
Point is: people can't be trusted to value anything. Remember that idiotic book Nudge? Look where it got us.
II.
You may want to ask whether "what constitutes a disease?" is something you really want the answer to. If it turns out that alcoholism is not a disease, then what? Close all the rehabs?
Trying to determine what is, or what is not, a disease is a distraction, a red herring. The real question is, what are we going to do about that thing?
The Average Joe is at a bit of a disadvantage. He feels something's amiss with say, "ADHD is a disease" but doesn't have the language to articulate it. So he says, "ADHD isn't a disease because it's too vague, not based on any physical pathology." He says that, because he's trying to argue like he thinks a doctor might argue, using the word "pathology" or using definitions. Consequently, his perfectly legitimate suspicion is dismissed, because his arguments seem weak to a doctor.
He needs to be true to himself. He doesn't need to argue it on doctors' terms, doctors need to argue it on his terms, because it's a social problem, not a scientific one.
His real problem with the diagnosis is what he's actually best suited to speak about: the social ramifications. "If you call ADHD a diagnosis, does that mean he gets extra time on the test and I don't?" That's the part that matters. Whether ADHD is "real" or not, whether there is a gigantic gaping pus hole in a "patient's" brain where something important should be is not what matters to Joe. What matters is, "he got this far even with the pus hole, why should he get a leg up just because he can't do as well as I can?"
Pies tries to argue like a doctor, because he thinks this is going to be decided by doctors. He doesn't realize that it has already been decided, by forces larger than him and Joe.
As if to reinforce that point, here is the advertisement found between Pies's article:
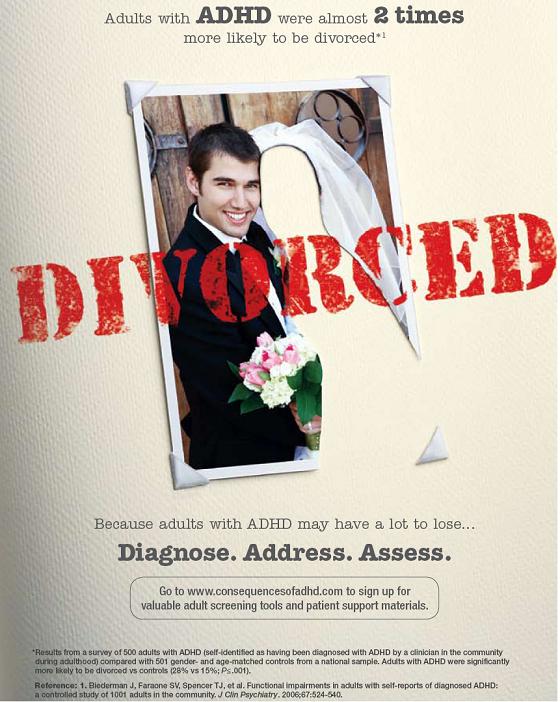 There's a social problem masquerading as a medical problem. Oh, you think it's a Pharma ploy to make money? Nope. Society wanted Pharma to take this problem off their hands. If you're wtaching it, it's for you.
There's a social problem masquerading as a medical problem. Oh, you think it's a Pharma ploy to make money? Nope. Society wanted Pharma to take this problem off their hands. If you're wtaching it, it's for you.
So what if it's true? Do we believe that treating ADHD will lower the divorce rate? Should having ADHD mean you get to keep the boat?
No one would dispute that the symptoms of ADHD exist, or even that they cluster together, or that they respond to Dexedrine. It's probably likely this is related to some physical change. But? What does having this mean? Does it mean society is obligated to pay for it? Defer to it? Those are the questions that matter, not whether it is a "disease."
The word "disease" is a safe house, it's "base." It's a clever accounting trick. Since "diseases" are defined to be value neutral and require both money and deference, rather than argue whether ADHD is worth our money and time, instead argue whether it is a disease. Once it gets labeled as a disease, no further arguments are necessary-- it's a disease. Don't be a heartless jerk. Step aside.
That drives Joe bananas. And it should.
This is not a failing of Pies; there's no possible way he could be expected to come up with a concrete solution. But his answer is just as ambiguous, relative, and subject to individual prejudices as simply defining a disease as "anything in which the person or surrounding people feel suffering. Severity of illness correlates to amount of suffering."
I'm not saying my definition is better-- it's equally valid, or invalid, or whatever you want to believe this whole project is.
It should be fairly obvious that "disease" is an entirely subjective term that can be applied legitimately to anything. "The disease of right wing conservative ideology." See? 50% of you agreed. Not jokingly agreed, mind you-- but found a serious element of truth to that diagnosis.
Point is: people can't be trusted to value anything. Remember that idiotic book Nudge? Look where it got us.
II.
You may want to ask whether "what constitutes a disease?" is something you really want the answer to. If it turns out that alcoholism is not a disease, then what? Close all the rehabs?
Trying to determine what is, or what is not, a disease is a distraction, a red herring. The real question is, what are we going to do about that thing?
The Average Joe is at a bit of a disadvantage. He feels something's amiss with say, "ADHD is a disease" but doesn't have the language to articulate it. So he says, "ADHD isn't a disease because it's too vague, not based on any physical pathology." He says that, because he's trying to argue like he thinks a doctor might argue, using the word "pathology" or using definitions. Consequently, his perfectly legitimate suspicion is dismissed, because his arguments seem weak to a doctor.
He needs to be true to himself. He doesn't need to argue it on doctors' terms, doctors need to argue it on his terms, because it's a social problem, not a scientific one.
His real problem with the diagnosis is what he's actually best suited to speak about: the social ramifications. "If you call ADHD a diagnosis, does that mean he gets extra time on the test and I don't?" That's the part that matters. Whether ADHD is "real" or not, whether there is a gigantic gaping pus hole in a "patient's" brain where something important should be is not what matters to Joe. What matters is, "he got this far even with the pus hole, why should he get a leg up just because he can't do as well as I can?"
Pies tries to argue like a doctor, because he thinks this is going to be decided by doctors. He doesn't realize that it has already been decided, by forces larger than him and Joe.
As if to reinforce that point, here is the advertisement found between Pies's article:
There's a social problem masquerading as a medical problem. Oh, you think it's a Pharma ploy to make money? Nope. Society wanted Pharma to take this problem off their hands. If you're wtaching it, it's for you.So what if it's true? Do we believe that treating ADHD will lower the divorce rate? Should having ADHD mean you get to keep the boat?
No one would dispute that the symptoms of ADHD exist, or even that they cluster together, or that they respond to Dexedrine. It's probably likely this is related to some physical change. But? What does having this mean? Does it mean society is obligated to pay for it? Defer to it? Those are the questions that matter, not whether it is a "disease."
The word "disease" is a safe house, it's "base." It's a clever accounting trick. Since "diseases" are defined to be value neutral and require both money and deference, rather than argue whether ADHD is worth our money and time, instead argue whether it is a disease. Once it gets labeled as a disease, no further arguments are necessary-- it's a disease. Don't be a heartless jerk. Step aside.
That drives Joe bananas. And it should.
![]() Digg |
Digg | ![]() del.icio.us |
del.icio.us | ![]() StumbleUpon |
StumbleUpon | ![]() Reddit |
Reddit | ![]() Yahoo! |
Yahoo! | ![]() My favourites
My favourites
24 Comments