No, Not Effexor, Too!? The Most Important Article On Psychiatry You'll Ever Read, Part II

In which Anne Neville agrees to believe pretty much anything anyone ever tells her, ever, and Richard discovers people are gullible idiots.
Go back and read Part I. Hurry.
Let's review the idea of sequential binding. A drug with affinity for multiple receptors doesn't bind to all of them simultaneously, but rather sequentially, like an aging polygamist, starting with the system for which it has the greatest affinity. Eventually, this maxes out, and it goes and adds the receptor system for which it has the second greatest affinity.
Once it has maxed out a receptor system, pushing the dose doesn't get you any more of that effect (or side effects.) You don't get less, but you don't get any more. You know what else is like that, sort of? Chlamydia.
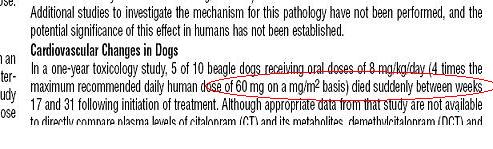
Let's look at an SSRI, Celexa. That first S stands for selective (serotonin reuptake inhibitor.) All of its clinical effect is coming from one single receptor system; this rum fountain has only one level-- and it's not that deep. By about 20mg, you've gotten as much serotonin effect as you are going to ever get.
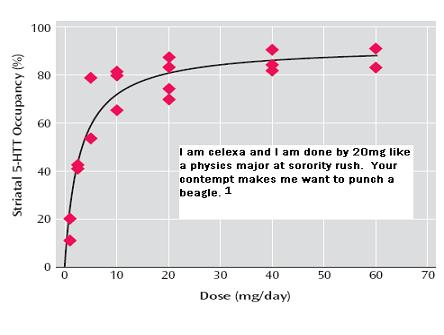
Certainly, by 40mg, you're all done. Do you expect the clinical difference from 10mg to 20mg to be significant? Maybe. How about 20mg to 40mg? Not so much. 40mg to 60mg? You woke me up for this? Don't touch me.
In other words, there's only one level in Celexa's rum fountain, and it's pretty much filled by 40mg. Pushing it to 60mg ("Now, with 50% more citalopram!") gets you a whole 3% more serotonin transporter binding. Which is embarrassing. I said don't touch me. Do it again and I'm calling an adult.
So what about Effexor, the serotonin/norepinephrine reuptake inhibitor, invented at Wyeth Labs by Kirsten Dunst, aka Vitamin C?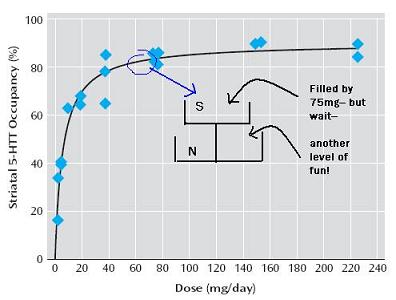
From the American Journal of Psychiatry study:
la, la, la , la , la, la ,la ,la ,la ,la
la ,la ,la,la, la,la
yeah, yeah, yeah,
la, la, la, la, la, la, [repeat x 36]
we will still be friends forever [sic]
Which is exactly the point. You don't get both S and N at all doses, it is, again, sequential: level 1 is S, maxed out by 75mg; and level 2 is N. Guess when level 2 (N) really kicks in? 150mg.
So anything after 150mg is really two systems at once, with the N increasing from there. 300mg is the same amount of S as 150mg, but the N is more.
Would you expect 75mg Effexor to be generally more efficacious than 40mg Celexa? No, because they are both doing the same thing: blocking about 80% of serotonin transporters. But what about after 150mg, when you have S and N?
From An Inconvenient Truth, 2006
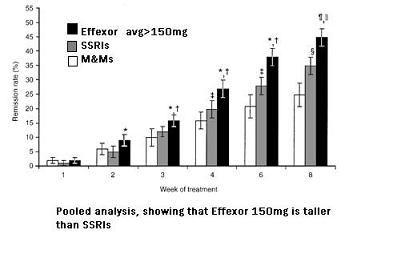
This is why Effexor studies only show superior efficacy at doses above 150mg-- because at 150mg, you start adding N on top of your already maxed out S. It's not adding more of the same drug, it is like adding a second drug. It's not more Effexor; it's taking a maxed out SSRI, and adding a NRI. It's like being with Princess Leia, but then adding Princess Ardala. And if you understood that joke, you should put down Yars' Revenge and kill yourself.
Let me be clear: I'm not saying Effexor is or is not better than an SSRI. I am saying that
- it would be impossible for it to be better then SSRIs, across a population, at less than 150mg.
- if it is going to be better, it would be better after 150mg, and only because you are adding a second system.
- If you are a doctor who "went all the way" up to 75mg Effexor for depression (or 300mg Seroquel for psychosis, etc, etc) and then stopped it because "it wasn't helping at all" then you should probably punch yourself in the testicles/uterus, you have missed the point. How one responds at 75mg IS NOT AT ALL PREDICTIVE of what might happen at 150 or more (or, for Seroquel and psychosis, 500mg or more) again, and for the last time, because higher doses aren't more, they are different.(2)
You can see this most clearly if you look at an MRI:
which is self-explanatory.(3)
What you may want to ask is this: why haven't you heard this stuff before? You think I discovered all this, in my basement lab, the one I use to create Jessica Simpson clones? I'm the Ponce de Leon of psychiatry?(4) Why the accepted delusion that a drug is the same, regardless of dose? Perhaps it's because this supposedly only applies to the newer drugs? The old ones-- Thorazine, Elavil, Pamelor, Remeron, Wellbutrin-- all blunt instruments, single receptor system drugs?
Why do we think that an inanimate object has a fixed identity, when even a person doesn't?
Next up: Aren't Two Drugs Better Than One?
--------
1. From the Celexa package insert: (warning: PDF-- clear your schedule)
2. Punching yourself in the testicles/uterus is not likely to help you learn this, it is more for my benefit.
3. It's technically an fMRI, bt the point is the same.
4. Ponce de Leon did not actually discover psychiatry, but he was the first to make it available to the masses.
IF YOU LIKE IT, DIGG IT, OR SEND ME RUM--
![]() Digg |
Digg | ![]() del.icio.us |
del.icio.us | ![]() StumbleUpon |
StumbleUpon | ![]() Reddit |
Reddit | ![]() Yahoo! |
Yahoo! | ![]() My favourites
My favourites
38 Comments