The Most Important Article On Psychiatry You Will Ever Read

I'm warning you.
Let's begin with a simple drive down a country road, say, I10.

The Three Problems of Psychiatry:
You know those white dashed lines separating the lanes in a highway? How long are they? Answer: _____________ Most people I ask say 3 feet. The real answer is 10 feet. Surprised? And that’s the first problem in psychiatry: perspective. Your perspective is always driving at 60mph, so they look 3 feet long. Unless you change your perspective, you never get to see the truth. Worse, much worse, you go through life confident they are three feet.
Which brings us to the second problem: closed mindedness. Even though I’ve told you the truth, you still don’t believe it—that’s how powerful your perspective is. “He must be talking about some other lines, maybe in France?” Unless you change your perspective, you will never be open to the truth, to the discovery that what you have thought, for your entire life, is wrong. Unless you get out of your car and measure those lines, you’ll never accept the truth.
Which brings us to the third problem: if you do try and change your perspective, get out and measure those lines, you will be quickly dispatched by a minivan to the face for your lack of faith.

The irony of it all was not lost on Paris. Or was it coincidence? Irony?
Here is a picture of a molecule of Seroquel:

It’s a single molecule. Count them.
Seroquel, like all atypical antipsychotics, binds to multiple receptor types. Seroquel blocks, with varying affinity, histamine (H1), alpha 1 (a1), dopamine (D2), etc, etc. You can imagine a molecule having different spokes to it, that each bind to different receptors. Here’s a graphical representation of this, made famous by Steven Stahl, MD, at the University of California, and formerly with Styx:

Consult your doctor if you are at risk for esophageal rupture
The other way this is often represented is with a pie chart:

From the video Serocool (Styx, 1981)
A typical understanding of this pie chart is that the various sizes represent “amounts” of blockade. So, here, Seroquel is very antihistaminergic—so it causes a lot of sedation. It is moderately an alpha1 blocker—which is what causes orthostasis (lightheadedness/dizziness/grogginess). And much less of a D2 blocker, which is what actually provides the antipsychotic effect. You can also see that Seroquel’s H1 section is bigger than Zyprexa’s, which explains why Seroquel is more sedating than Zyprexa. (1)
One molecule gets you H1, a1, 5HT2a, D2
Two molecules gets you twice as much H1, a1, 5HT2a, D2
So this is so easy to visualize that anyone can understand it. But unfortunately this representation is misleading, it leads you to think something that is not completely accurate, in the same way that looking at Nancy Pelosi makes you think of that guy in Raiders of the Lost Ark:

BUT HOW CAN COLOR PICTURES BE WRONG?
One of the central themes of the postmodern critique of our values is that aesthetics must trump truth as long as aesthetics remains undefined. That’s the semiotic conundrum, why psychiatry is politics: the truth is demanded only when it supports a preset ideology.
WHAT THE HELL ARE YOU TALKING ABOUT?
Nothing. Let’s move on.
The mistake is that those pie chart sections aren’t amounts, they are affinities. They are preferences. Here's a metaphor. Imagine you have only one molecule of Seroquel. Where does one single molecule prefer to go? It can’t go to four different places, right? It has to "choose." And most likely it chooses to go to H1. The spokes don't cause the effect-- the spokes fit into receptors-- the receptor causes the effect. So if it binds to H1 receptor, the other spokes remain unused.
Let’s say you are a gentleman, and as such prefer blondes by virtue of their fair hair, lithe contouring, and receptiveness to new ideas. If you’re in a room with 10 brunettes and two blondes, do you go to everyone, equally? (Assume for this gedankenexperiment you have only the one, non-mechanical penis.) No, you make a bee line for the blondes.

Tom was thankful he was sober enough to avoid the ugly one
WHAT IF ALL THE BLONDES ARE TAKEN?
This is a safe bet. Sadly, since not every blonde will support your ideas for a ménage, you’ll have to settle for the brunettes. Painful, I know. I can call you in a script for Viagra.
So one molecule goes to H1. What about two molecules? Or three? Or 13 gazillion?
Think how sedating 25mg of Seroquel is (trust me, it's sedating.) Why isn't 32 times more-- 800mg-- lethal? Certainly 32mg of Xanax is more than a short nap, so what's the difference?
Instead of thinking that the drug binds to all receptors simultaneously, a better analogy would be a champagne fountain, like at a wedding. Except I hate champagne, so pretend it is a rum fountain. Rum fills the top level, overflows into the second level, then that overflows into the third, etc. You can't get anything into level 3 until you fill levels 1 and 2. And, once you've filled level 1, you can't put anything more into it.

Get it? So level one can be labeled H1, level two is alpha 1, and level 3 is D2. (2)
So you can see that, at some dose, there is no more increasing sedation with Seroquel. You've filled up level 1-- the H1 section. Going from 25mg to 50mg is a big jump in sedation (level 1), but going from 400mg (level 3) to 800mg is not felt to be an increase in sedation. It's the same amount of sedation, because by the time you hit 400mg, you were all full up. (3)
But there’s a dark side to my analogy, and it isn’t the rum fits. Here’s the thing: if one molecule of Seroquel goes to H1, and not to D2, then can it have any antipsychotic effect? No. One molecule binds to H1, so it isn't an antipsychotic, it's an antihistamine.
DOESN’T THE BOX CLEARLY SAY ANTIPSYCHOTIC?
Yes, it does. Weird, isn’t it?
Until this drug is blocking a significant number of D2 receptors, it is not functioning as an antipsychotic. Important: the antipsychotic effect of one molecule of Seroquel isn't so weak you just can't see it-- it is exactly and precisely zero.
The drug can't be called an antipsychotic unless it is behaving as an antipsychotic, regardless of the product labeling.
ARE YOU SAYING THE FDA ARE A BUNCH OF UNSCIENTIFIC ASS-MONKEYS?
What?
At some amount of D2 blockade, these things will be antipsychotics. What amount? Theories abound, but look at it this way: 10mg of Zyprexa blocks a certain number of D2 receptors. How much Seroquel, Risperdal, or Geodon does it take to block the same number? Answer:
10mg Zyprexa = 500mg Seroquel = 3mg Risperdal= 120mg Geodon. (4)
This is the problem so many doctors have. “I tried him on Seroquel, it didn’t work.” Really? At what dose? Because higher doses aren’t stronger—they are completely different. The behavior of Seroquel at 100mg is completely different than the behavior and effects at 500mg. 500mg is an antipsychotic; 100mg is not an antipsychotic. I know it looks like it’s five times more, but it’s not—it’s the addition of a completely new level. It's like adding a new “drug.” Just because the FDA calls it an antipsychotic, and that word is printed on the box, doesn't mean it is.
DOES THAT MEAN 5mg ZYPREXA = 250mg SEROQUEL?
So you weren’t listening.
Reducing these doses by half pretty much extinguishes the D2 blockade. Reducing the dose puts you into a different "level." They’re not half as good as they were, they’re completely different.
The drug isn't a tease. It doesn’t give you a little bit of efficacy at a low dose, “oh, it’s working a little bit—he must be a Seroquel responder—I’ll just increase the dose to get more efficacy.” Another way of saying it is this: the absence of efficacy at 250mg is in no way predictive of what might happen at 500mg, because the two doses are working at different receptors.
So, yes, 5mg Zyprexa is equal to 250mg Seroquel for psychosis, in the same way that an academic psychiatrist is like a certain Congresswoman from California: they all do nothing. ZING! (5)
Next up: Oh, No, Not Effexor, Too?
----------------------------------
1. The pie chart is wrong, wrong in the same way that Pamela Anderson is wrong, i.e. right in many ways. This is an in vitro pie chart, derived from affinities of receptors ripped out of the cadaverous remains of former tax attorneys. It may not represent what happens in an actual human body when confronted with unequal distribution of drug and receptors, number, and subtypes of receptors. It also doesn’t account for competition from other endogenous chemicals, drugs, or ice picks in the skull. All this notwithstanding, they are still usefully inaccurate. And all this is just a metaphor anyway.
2. This is not technically accurate. Receptor systems don’t fill up, i.e. become saturated, before the next system is impacted. More accurately, there exists a certain level of binding at one receptor such that it then becomes equally likely that it goes elsewhere. So my rum fountain should be more accurately labeled “the effects from H1 blockade” and “the effects from alpha 1 blockade.” Those effects do “max out.” Also, a drug’s maximal effect can occur well before 100% saturation of a system; for example, 10% H1 blockade may be all that is necessary to get maximal sedation, such that increasing binding to 20% doesn’t get you more effect. Nor might a drug be able to bind to more than 10%. So while binding saturation is often used interchangeably with maximal effect, they are not the same.
3. Drugs bind to specific receptors, but also nonspecifically (i.e. everywhere else.)
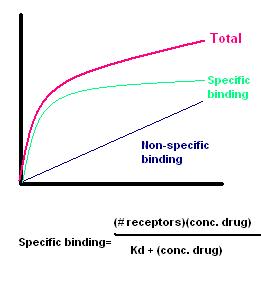
Note that binding is related to the rates of the binding (Kd=Koff/kon)
If you want a real world example, look at Zyprexa, below-- a real human in a real PET scanner eating real Zyprexa:
If you increase the dose from 5mg to 30mg, serotonin binding increases from 95% to 100%. Do you expect to “feel” much difference? But D2 binding goes from 55% to 85%. That you’ll feel.)
4. Be careful: these are the equivalents for D2 blockade—for antipsychosis. If you are using Zyprexa for, say, anxiety, then maybe D2 isn’t the relevant system. Maybe it’s the serotonin that’s relevant. (I have no idea; NO ONE HAS ANY IDEA.) So the conversion doesn’t hold. Do you understand? If you are using 10mg Zyprexa tablets to clog a toilet in some heroin fueled Consumer Reports product test down at the American Standard offices, you don’t need 500mg Seroquels to get the same clogging action. Ok?
5. Actually, this isn’t true either. 250mg Seroquel has trivial D2 blockade, but Zyprexa 5mg still has some (55%). So 5mg Zyprexa is more likely to treat psychosis than 250mg Seroquel. The equivalences are really to be used the other direction: if you needed 15mg of Zypexa, you will likely need more than 600mg Seroquel…
IF YOU LIKE IT, DIGG IT-- OR REDDIT IT-- OR SEND ME MONEY-- OR RUM--
![]() Digg |
Digg | ![]() del.icio.us |
del.icio.us | ![]() StumbleUpon |
StumbleUpon | ![]() Reddit |
Reddit | ![]() Yahoo! |
Yahoo! | ![]() My favourites
My favourites
85 Comments