February 22, 2010
How Seroquel XR Works, Part 2
The ongoing story of a government cover-up
Part 1 was here.
Let's assume it did bind to the NET, how much of the efficacy should we attribute to norepinephrine?
In the pre/frontal cortex there are no pure dopamine transporters (DAT), and the NET is primarily responsible for dopamine's reuptake. So the NET, which norquetiapine fully occupies/barely touches, transports about 50/50 norepinephrine and dopamine.
So even if the NET is inhibited, the ultimate effect in the frontal lobe may be related to dopamine.
Are there any other better explanations for Seroquel's antidepressant efficacy?
It's odd that while the FDA has chosen to be unsure about the mechanism of action in psychosis, it is confident in the MOA in depression. Here are some equally/more likely explanations for the antidepressant effect:
H1 antagonism: sure, why not? 6 points on a Hamilton for sleep, another 2 for weight gain...
Partial agonism at 5HT1a: Think Buspar.
a2 antagonism: (inhibitory autoreceptors.) Blocking these would increase serotonin and norepinephrine release, etc.
Unfortunately, a2 antagonism is a property only of quetiapine, not norquetiapine.
Why is that unfortunate?
Because if norquetiapine is marketed as a new drug...
But if norquetiapine does actually inhibit the NET, wouldn't that at least be a plausible mechanism for its efficacy? Since Effexor and Cymbalta work...
I'll grant that it is evident Effexor and Cymbalta work; but who are you asking to tell you why they work? Wyeth and Lilly? That's like asking your future wife's ex-boyfriends to write her a letter of recommendation. "She's so awesome, she'll make you really happy." Oh, I guess I should go shave my back then.
That's a very disturbing visual, Backbeard.
Let's do an abbreviated analysis for Effexor. According to this non-porn site, the Ki for the SERT is 80nM and NET 3000nM (1000-6000). This means it "prefers" to go to the serotonin transporter (SERT).
Consistent with this is PET data showing high SERT binding in striatum:
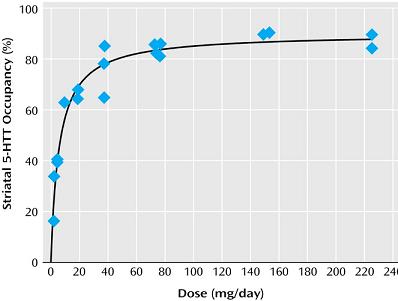
This is a comforting graph, and shows the "fountain" approach to understanding a "dirty" drug's effects. But note that the line isn't flat, it still trends upwards. If the affinity for the SERT is 200-600 times that for NET, then clinically meaningful effects on NET would have resulted in serotonin overload.
But that's speculation. You've already shown that the Ki's are unreliable guides of in-vivo affinities and effects.
Ok:
What you want is a direct test of the operation of the NET in the human body.
If you inject tyramine into your friend, it will be taken up into the presynaptic NE terminal by the NET, where it will cause the release of norepinphrine. The blood pressure then reliably goes up.
If you block the NET, this effect will also be blocked, since tyramine can't get in. Nortriptyline, a tricyclic and "norepinephrine reuptake inhibitor" blocks the tyramine effect almost completely.(1)
What about Effexor? If Effexor is an NRI, it should also block the blood pressure elevation. Zoloft, not an NRI, should not block it-- the BP should go up.
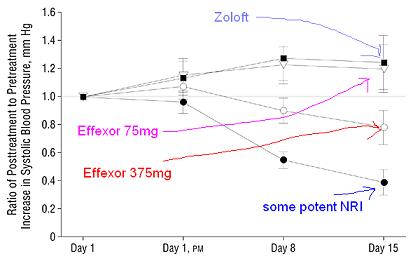
This is ratio of post/pre blood pressures; >1 means tyramine caused BP to go up, <1 means tyramine couldn't get BP to go up.
What you see is that 75mg of Effexor was no more an NRI than Zoloft; and maprotiline (the NRI) turned Effexor 375mg into a cuckold.
But surely Cymbalta has impressive clinically relevant NRI effects?
What dose of tyramine is needed to make the BP go up 30mmHg? That's called the PD30. If a drug blocks the effect (like desipramine, an NRI, would) than it would take more a higher dose of tyramine:
Well that's unfortunate. (2)
But then how can they claim Cymbalta is an NET?
1. By ki, the SERT/NET ratio is about 10, versus Effexor's 200, so in that sense you get the norepinephrine "earlier" in the dosing cycle;
2. If it blocks the NET, then it should also decrease the cycle of norepinephrine turnover (since it isn't being taken back up and degraded.) So there should be less NE and its metabolites in the urine. And that's certainly what this study finds (abstract:)
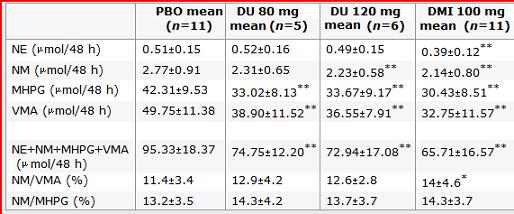 Compare the NRI desipramine (DMI) to placebo, note the decrease in urine NE and metabolites. You can see that while the levels of NE and its metabolites decreased in the urine, Cymbalta resulted in a decrease in only the metabolites, but not NE itself. Do you know why? No one else does either.
Compare the NRI desipramine (DMI) to placebo, note the decrease in urine NE and metabolites. You can see that while the levels of NE and its metabolites decreased in the urine, Cymbalta resulted in a decrease in only the metabolites, but not NE itself. Do you know why? No one else does either.
On the basis of this study we can reasonably conclude only that duloxetine is spelled with an x.
So you're saying that they arbitrarily decided on the mechanism of action of Seroquel by its barely detectable similarity to Effexor and Cymbalta, which themselves don't generate their efficacy the way they say they do and Seroquel hoped they did?
At this point, someone in the room should probably say "oops."
-----
Part 3. (You mean there's a Part 3?)
----
1. One interesting conclusion of this is that it would therefore be safe to mix an MAOI with Pamelor. THAT IS NOT A CLINICAL RECOMMENDATION.
2. If you want to make a gazillion dollars, perform the TYR30 test with Seroquel and norquetiapine. Residents: I just gave you a treasure map.
Let's assume it did bind to the NET, how much of the efficacy should we attribute to norepinephrine?
In the pre/frontal cortex there are no pure dopamine transporters (DAT), and the NET is primarily responsible for dopamine's reuptake. So the NET, which norquetiapine fully occupies/barely touches, transports about 50/50 norepinephrine and dopamine.
So even if the NET is inhibited, the ultimate effect in the frontal lobe may be related to dopamine.
Are there any other better explanations for Seroquel's antidepressant efficacy?
It's odd that while the FDA has chosen to be unsure about the mechanism of action in psychosis, it is confident in the MOA in depression. Here are some equally/more likely explanations for the antidepressant effect:
H1 antagonism: sure, why not? 6 points on a Hamilton for sleep, another 2 for weight gain...
Partial agonism at 5HT1a: Think Buspar.
a2 antagonism: (inhibitory autoreceptors.) Blocking these would increase serotonin and norepinephrine release, etc.
Unfortunately, a2 antagonism is a property only of quetiapine, not norquetiapine.
Why is that unfortunate?
Because if norquetiapine is marketed as a new drug...
But if norquetiapine does actually inhibit the NET, wouldn't that at least be a plausible mechanism for its efficacy? Since Effexor and Cymbalta work...
I'll grant that it is evident Effexor and Cymbalta work; but who are you asking to tell you why they work? Wyeth and Lilly? That's like asking your future wife's ex-boyfriends to write her a letter of recommendation. "She's so awesome, she'll make you really happy." Oh, I guess I should go shave my back then.
That's a very disturbing visual, Backbeard.
Let's do an abbreviated analysis for Effexor. According to this non-porn site, the Ki for the SERT is 80nM and NET 3000nM (1000-6000). This means it "prefers" to go to the serotonin transporter (SERT).
Consistent with this is PET data showing high SERT binding in striatum:
This is a comforting graph, and shows the "fountain" approach to understanding a "dirty" drug's effects. But note that the line isn't flat, it still trends upwards. If the affinity for the SERT is 200-600 times that for NET, then clinically meaningful effects on NET would have resulted in serotonin overload.
But that's speculation. You've already shown that the Ki's are unreliable guides of in-vivo affinities and effects.
Ok:
What you want is a direct test of the operation of the NET in the human body.
If you inject tyramine into your friend, it will be taken up into the presynaptic NE terminal by the NET, where it will cause the release of norepinphrine. The blood pressure then reliably goes up.
If you block the NET, this effect will also be blocked, since tyramine can't get in. Nortriptyline, a tricyclic and "norepinephrine reuptake inhibitor" blocks the tyramine effect almost completely.(1)
What about Effexor? If Effexor is an NRI, it should also block the blood pressure elevation. Zoloft, not an NRI, should not block it-- the BP should go up.
This is ratio of post/pre blood pressures; >1 means tyramine caused BP to go up, <1 means tyramine couldn't get BP to go up.
What you see is that 75mg of Effexor was no more an NRI than Zoloft; and maprotiline (the NRI) turned Effexor 375mg into a cuckold.
But surely Cymbalta has impressive clinically relevant NRI effects?
What dose of tyramine is needed to make the BP go up 30mmHg? That's called the PD30. If a drug blocks the effect (like desipramine, an NRI, would) than it would take more a higher dose of tyramine:
| TYR PD30 (mg) | ||
|---|---|---|
| Day 7 | Day 8 | |
| Placebo (n=12) | 7 [4-14] | 6 [5-9] |
| Duloxetine 80 mg (n=5) | 9 [5-8] | 7 [4-7] |
| Duloxetine 120 mg (n=6) | 6 [5-9] | 4 [4-7] |
| Desipramine 100 mg (n=11) | 30 [22-82] | 18 [12-31] |
Well that's unfortunate. (2)
But then how can they claim Cymbalta is an NET?
1. By ki, the SERT/NET ratio is about 10, versus Effexor's 200, so in that sense you get the norepinephrine "earlier" in the dosing cycle;
2. If it blocks the NET, then it should also decrease the cycle of norepinephrine turnover (since it isn't being taken back up and degraded.) So there should be less NE and its metabolites in the urine. And that's certainly what this study finds (abstract:)
Urinary and cardiovascular measurements suggest that duloxetine has an effect on NE synthesis and turnover, indicative of NE reuptake inhibition."Suggest?"
Compare the NRI desipramine (DMI) to placebo, note the decrease in urine NE and metabolites. You can see that while the levels of NE and its metabolites decreased in the urine, Cymbalta resulted in a decrease in only the metabolites, but not NE itself. Do you know why? No one else does either. On the basis of this study we can reasonably conclude only that duloxetine is spelled with an x.
So you're saying that they arbitrarily decided on the mechanism of action of Seroquel by its barely detectable similarity to Effexor and Cymbalta, which themselves don't generate their efficacy the way they say they do and Seroquel hoped they did?
At this point, someone in the room should probably say "oops."
-----
Part 3. (You mean there's a Part 3?)
----
1. One interesting conclusion of this is that it would therefore be safe to mix an MAOI with Pamelor. THAT IS NOT A CLINICAL RECOMMENDATION.
2. If you want to make a gazillion dollars, perform the TYR30 test with Seroquel and norquetiapine. Residents: I just gave you a treasure map.
![]() Digg |
Digg | ![]() del.icio.us |
del.icio.us | ![]() StumbleUpon |
StumbleUpon | ![]() Reddit |
Reddit | ![]() Yahoo! |
Yahoo! | ![]() My favourites
My favourites
32 Comments